Treatment proposal and drainage protocol
The earlier in the course of the disease the catheter is inserted, the greater the benefit is to the patient.
International guidelines for malignant pleural effusion and malignant ascites clearly state that indwelling catheters should be considered for early treatment. The treatment method provides patients with effective symptom relief and saves hospital days. The cost will therefore be lower than for alternative treatment methods. Studies on benign pleural fluid and ascites also show good results.
Treatment options for malignant pleural effusion
Ascites catheter treatment suggestions
The earlier in the course of the disease the patient receives the catheter, the greater the benefit to the patient. A large study³ has chosen to implant the catheter without prior therapeutic paracentesis in patients with newly diagnosed malignant ascites with rapid accumulation, troublesome symptoms and poor quality of life. The reason for this is because repeated paracentesis (Large Volume Paracentesis = LVP) would be uncomfortable for the patient.
Furthermore, repetition of this procedure (LVP, editor’s note) leads to frequent hospital visits, which are inconvenient for the patient, entail the use of more healthcare resources, and may lead to delays in drainage resulting in patients becoming progressively symptomatic in the terminal stages of their illnesses. Given that over 80 percent of the patients in this study had poor performance status (an ECOG score of at least 3), in our clinic we used clinical judgement that the PleurX catheter would benefit the patient – rather than a history of therapeutic paracentesis – as another indication for catheter insertion. This was justified by the low rate of catheter removal (4,05%), as mentioned earlier³.
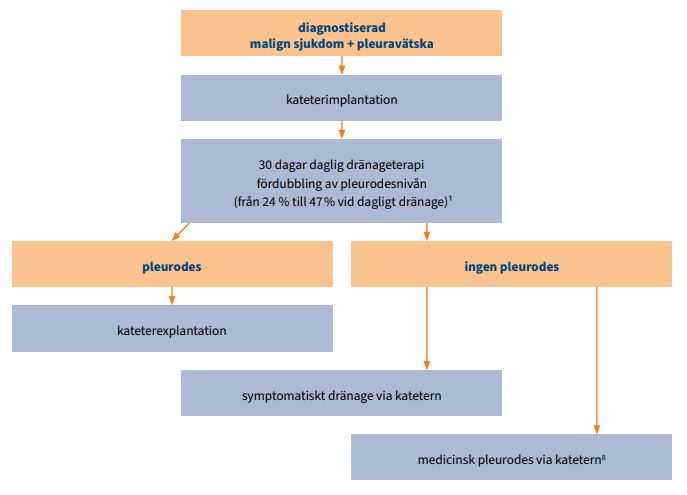
Suggested drainage protocol for pleural effusion
In case of pleurodesis prescription:
- Implant the catheter and drain as much as possible.
- The patient can be discharged the same day and drain 500 ml daily (alternatively up to a maximum of 1000 ml if the patient can tolerate it) with our drainage sets.
- If you drain less than 100 ml, you can reduce the drainage to every other day.
- If you drain less than 50 ml on 3 consecutive drainages, the patient probably has pleurodesis. Check with ultrasound or X-ray.
- In the case of confirmed pleurodesis, the choice of removing the catheter or keeping it can be made, depending on the patient’s preference or what is medically desirable.
For symptom relief:
- Drain 2-3 times a week (max 1000 ml), and more often if necessary, with our drainage sets.
- The drainage frequency can be decreased when fluid production is reduced, but not less than once a week.
- Note that there may be a pleurodesis despite infrequent drainage, see above.
Sources for drainage protocol for pleural effusion see references 1 and 2.
Suggested drainage protocol for ascites
- Implant the catheter and try to drain as empty as possible based on the patient’s medical conditions before the patient is discharged. Observe national guidelines for ascites drainage regarding possible albumin replacement.
- The patient can be discharged the same day and then drain a maximum of 2000 ml per day with our drainage sets.
- To avoid leakage, we recommend more frequent drainages in the first few weeks until there is tissue ingrowth around the catheter cuff .
- Drain 2-3 times a week, and more often if necessary, with our drainage sets.
Sources for drainage protocol for ascites see references 3 and 4.
Benefits for you as a treating physician:
- Saves medical time (no repeated procedures and associated risks)
- Cost reduction
- Faster start of therapy, in parallel with medical therapy and/or radiotherapy
Advantages for your patients:
- Improved quality of life and effective symptom relief
- No unnecessary procedures
- Reduction of hospital stays and visits to physician
References
- Wahidi et al., Randomized Trial of Pleural Fluid Drainage Frequency in Patients with Malignant Pleural Effusions. The ASAP Trial. American Journal of Respiratory and Critical Care Medicine. 2017; 195(8):1050-1057.
- Chalhoub et al., The Use of the PleurX Catheter in the Management of Non-Malignant Pleural Effusions, Chronic Respiratory Disease; 8(3): 185-191.
- Wong BCT et al., Indwelling Peritoneal Catheters for Managing Malignancy-Associated Ascites, Journal of Palliative Care 31:4 / 2015; 243-249.
- Nationell riktlinje 2016 på uppdrag av Svensk Gastroenterologisk Förenings styrelse: Ascites och njursvikt vid levercirros – utredning och behandling.
- Bhatnagar, Keenan, Morley, et al. Outpatient Talc Administration by Indwelling Pleural Catheter for Malignant Effusion. The New England Journal of Medicine. 2018; 378(14):1313-1322.
